Immune responses in health, disease and diagnosis

The immune system is complex. A finely tuned interplay between white cells, lymphoid tissue, antibodies, cytokines and other signalling pathways. When regulation fails, the consequences can be far-reaching.
Immune-mediated disease usually presents with non-specific clinical signs, reflecting disruption of different components of the immune system and a working understanding of how the immune system functions – and how it can malfunction – provides a useful framework for interpreting these cases and guiding diagnostic decision-making.
At its simplest, immune defence can be divided into two interconnected arms – innate and adaptive immunity.
Innate versus adaptive immunity
Innate immunity provides the body’s first line of defence. It is rapid and generally non-specific, relying on physical barriers such as the skin, mucous membranes, airways and the blood brain barrier, alongside inflammatory responses and the complement system.1 The innate immune response is efficient but indiscriminate, responding in much the same way to repeated challenges and without immunological memory.
Adaptive (acquired) immunity, by contrast, is slower to develop but very specific. It is mediated by B and T lymphocytes, with B cells producing antibodies directed against specific antigens, and T cells coordinating, amplifying or downregulating the immune response. Crucially, adaptive immunity is capable of memory, allowing a faster and more effective response on re-exposure. While this is essential for successful vaccination, for example, it also explains why inappropriate or misdirected adaptive immune responses can result in autoimmune and other immune-mediated disease.
The mucociliary escalator
One example of innate immunity is the mucociliary escalator of the respiratory tract. From the nasal passages to the bronchioles, the airway epithelium is lined with mucus-producing cells and cilia that act together to trap and remove inhaled particles, including dust, spores and infectious organisms.
This defence mechanism is highly effective but easily compromised. Poor ventilation, dusty environments, exposure to smoke and chronic airway disease can all impair mucociliary clearance and increase susceptibility to infection. Conditions such as primary ciliary dyskinesia will also negatively impact the mucociliary escalator.
Primary ciliary dyskinesia2
– Normally autosomal recessive condition
– All reported cases are in pedigree breeds including
– Border collies
– Golden retrievers
– Old English sheepdogs
– Treatment: symptomatic for recurrent bronchopneumonia
– Prognosis: guarded to poor
When immune regulation fails
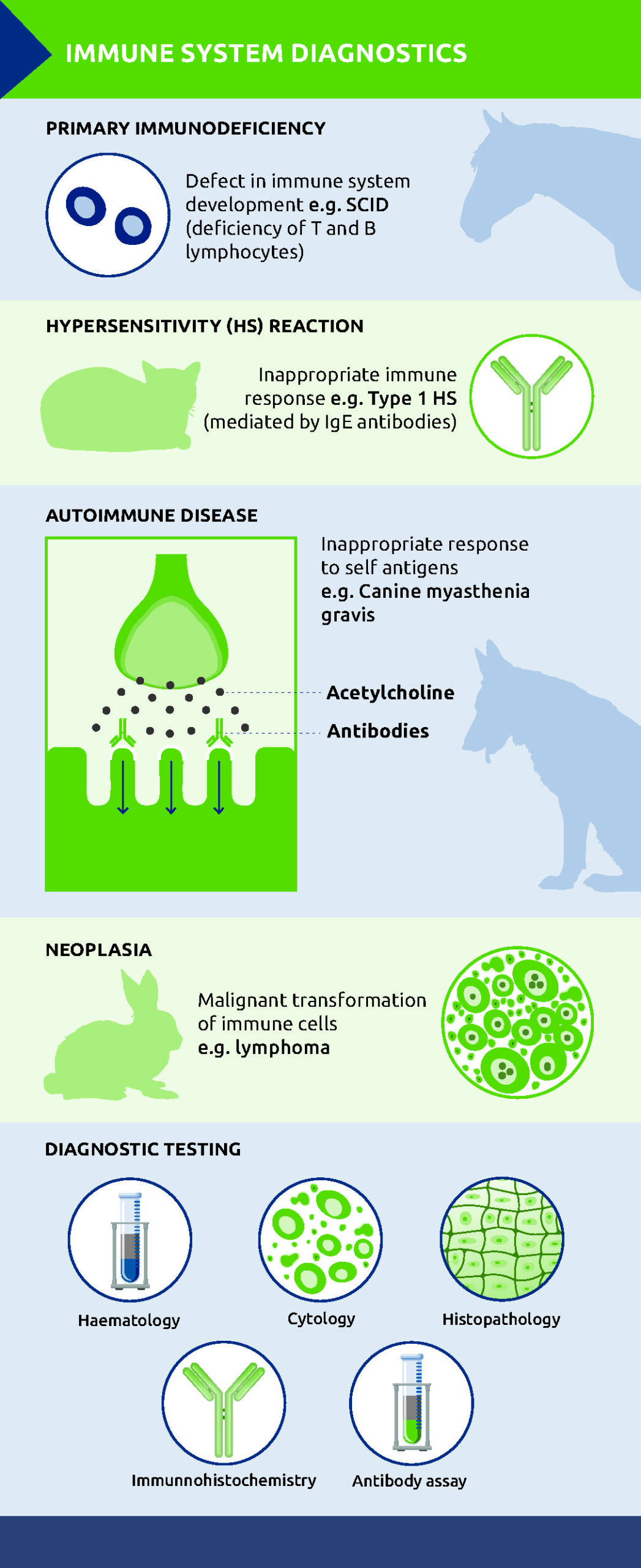
In clinical terms, disorders of the immune system broadly fall into four patterns:
– Immunodeficiency – an inadequate immune response
– Hypersensitivity – an excess or inappropriate response
– Autoimmune disease – loss of ability to distinguish between foreign and self antigens
– Neoplasia – malignant transformation of immune cells
Immunodeficiency
Immunodeficiency may be primary or secondary to various factors including age, malnutrition, chronic disease, or co-infections. Primary immunodeficiencies arise from intrinsic defects in immune system development, such as failure to produce functional stem cells or mature B or T lymphocytes.
Primary immunodeficiencies are rare, and are usually attributable to congenital defects in immune system components.3 Affected animals are more susceptible to infection from a young age and a well recognised example is severe combined immunodeficiency (SCID) in Arabian foals. This inherited autosomal recessive condition results from a genetic mutation affecting an enzyme critical to lymphocyte development, leading to a profound deficiency of T lymphocytes and a lack of functional B lymphocytes producing IgM. As a result, affected animals are unable to generate antigen-specific immune responses following infection or vaccination.4
Clinically, foals with SCID appear normal at birth due to passive transfer of maternal antibodies, but become increasingly susceptible to opportunistic infections as maternal immunity wanes. Most die by five to six months of age. Identification of carrier animals through genetic testing is therefore central to disease prevention
Hypersensitivity
In contrast, hypersensitivity reactions arise from exaggerated or inappropriate immune responses to antigens that would otherwise be harmless. These reactions are further categorised, with type 1 hypersensitivity perhaps the most commonly encountered in practice.
Type 1 hypersensitivity is mediated by IgE antibodies bound to mast cells. On re-exposure to an antigen, cross-linking of IgE molecules triggers mast cell degranulation, releasing histamine and other inflammatory mediators. The resulting clinical signs can range from localised pruritus and erythema to systemic effects, including anaphylaxis.5 While diagnosis is often based on history and clinical presentation, in some cases, allergy testing may be used alongside to help identify relevant allergens.
Autoimmune disease
While hypersensitivity reactions reflect excessive immune responses to external antigens, similar mechanisms can also be directed inappropriately against the body’s own tissues. Autoimmune disease arises when the immune system loses the ability to distinguish between self and non-self antigens, resulting in immune-mediated damage to the body’s own tissues. These conditions may be tissue-specific or systemic and often present with vague, fluctuating or progressive clinical signs, making diagnosis challenging. In many cases, routine diagnostics help exclude infectious or metabolic causes, but definitive diagnosis relies on targeted testing that reflects the underlying immune mechanism.
Canine myasthenia gravis
A useful example is acquired canine myasthenia gravis (cMG), an autoimmune disorder of neuromuscular transmission. In this condition, autoantibodies are directed against nicotinic acetylcholine receptors at the neuromuscular junction,6 impairing signal transmission between nerves and muscles. Clinically, dogs may present with focal disease, commonly manifesting as megaoesophagus due to weakness of the oesophageal, pharyngeal and facial muscles, or with generalised weakness that worsens with exercise. Acetylcholine receptor antibodies (ACRABs) can be used for diagnosis, with a positive serum titre for ACRABs highly suggestive of acquired cMG.
Masticatory muscle myositis
Masticatory muscle myositis provides another illustration of tissue-specific autoimmunity. The masticatory muscles are predominantly composed of Type 2M fibres and the disease is characterised by the production of autoantibodies against these fibres.7 Affected dogs may present with pain on opening the mouth, trismus or progressive temporal muscle atrophy.
Serum assay for autoantibodies against Type 2M fibres can support diagnosis. However, false negative results may be obtained if immunosuppressive dosages of corticosteroids have been given for longer than seven to ten days, in end-stage masticatory muscle myositis and in polymyositis. In these cases, a muscle biopsy may be indicated.
Neoplasia of the immune system
Disorders of the immune system are not limited to dysregulation of immune responses; immune cells themselves may become neoplastic. Lymphoma and leukaemia arise from malignant transformation of lymphoid cells and diagnosis typically relies on a combination of cytology, histopathology and in some cases, immunophenotyping to determine cell lineage and determine prognosis.
Mast cell tumours are another common diagnosis. Mast cells play a central role in Type I hypersensitivity reactions through IgE-mediated degranulation, yet when neoplastic, they can give rise to tumours with highly variable behaviour. Clinical signs may be disproportionate to tumour size due to the systemic effects of histamine and other inflammatory mediators.
There is no doubt that immune-mediated disease remains one of the more diagnostically challenging areas of clinical practice. Used appropriately, laboratory testing can support clinical decision-making by clarifying underlying mechanisms and diagnostic limitations. Close collaboration with a diagnostic laboratory can be invaluable, helping ensure that test selection, timing and interpretation maximise diagnostic yield and improve patient outcomes.
References
1. Wang, R. et al. (2024) The interaction of innate immune and adaptive immune system. MedComm. 5:e714. https://doi.org/10.1002/mco2.714
2. Braund, K. & Blake, R. (online) Primary ciliary dyskinesia. In: Vetlexicon Canis. ISSN 2398-2942. Vetstream Ltd, UK.
3. Swann, J.W. (2025). Primary Immunodeficiencies. In Veterinary Clinical Immunology (eds O.A. Garden and L. Kidd). https://doi.org/10.1002/9781119232957.ch18
4. Coyne, C., Holmes, M., Menzies-Gow, N. Vetstream Ltd & Prof Derek Knottenbelt (online) Immunology: combined immunodeficiency. In: Vetlexicon Equis. ISSN 2398-2977. Vetstream Ltd, UK.
5. Tizard, I. (2025) Hypersensitivity Diseases in Animals. MSD Veterinary Manual. Hypersensitivity Diseases in Animals – Immune System – MSD Veterinary Manual
6. Downey Koos, L. (2024) Acquired Myasthenia Gravis in Companion Animals. Todays Veterinary Practice. TVP-2024-1112_Myasthenia-Gravis.pdf
7. Di Tosto, M. et al. (2022) Case report: Atypical and chronic masticatory muscle myositis in a 5-month old Cavalier King Charles Spaniel. Clinical and diagnostic findings, treatment and successful outcome. Front. Vet. Sci. Sec. Veterinary Neurology and Neurosurgery. Vol 9 https://doi.org/10.3389/fvets.2022.955758
Original publication: The Veterinary Edge, April 2026, pages 38-40
About the author
Sandra Dawson graduated from Aberdeen and Glasgow universities with degrees in agriculture and veterinary medicine. After working in mixed practice, she completed a residency in veterinary pathology at Edinburgh University, where she also lectured in reproductive pathology. Following five years in industry, during which she gained her FRCPath, Sandra joined NationWide Laboratories. In 2011, she was appointed to the Royal College of Pathologists board of examiners in the speciality of small domestic animals. Sandra specialises in histopathology, working with surgical biopsies and fine needle aspirates across a wide range of species.