The Case of the Collapsing Collie

Credit: Sandra Dawson BSc BVMS FRCPath MRCVS
Featuring: Ben (Sandra’s own companion)
Ben is an 11-year-old male neutered Border collie. He was rescued 5 years ago. He has been in good health but presented with a 36-hour history of collapse.
Clinical examination showed depression with pale mucous membranes and a tender abdomen. Ultrasound examination of the abdomen showed an enlarged irregular spleen with multifocal irregular areas.
Haematology showed a mild non-regenerative or pre-regenerative anaemia. Ben’s clinical condition was deteriorating so a decision was made to perform an exploratory laparotomy. The spleen was found to be enlarged and contained multiple, variably sized nodules (Fig.1). No other lesions were detected on surgical examination of the abdomen…

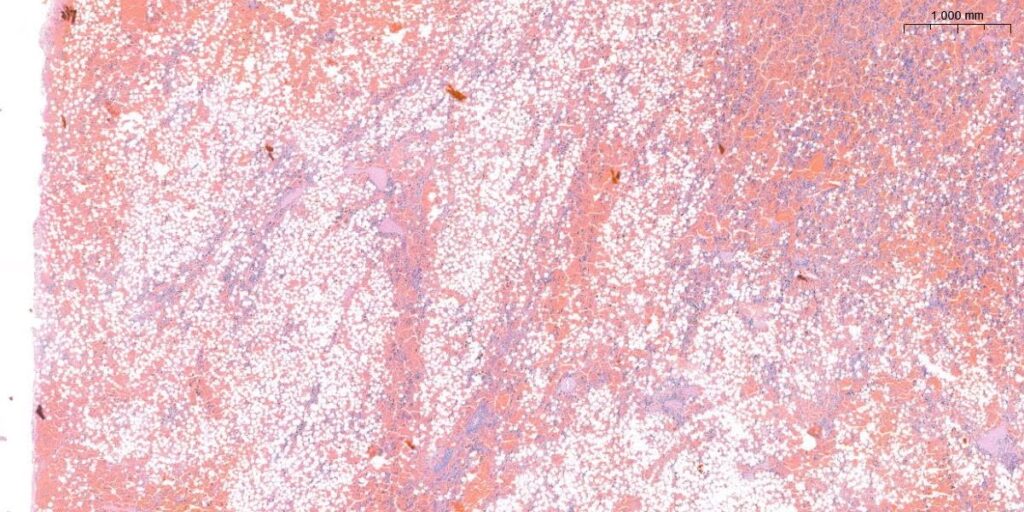
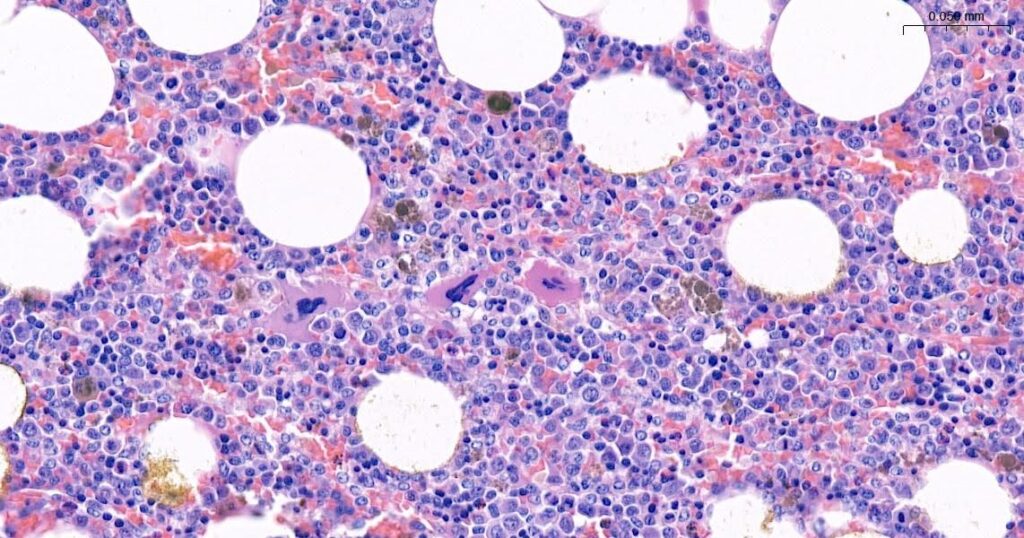
Multiple blocks of tissue were taken from various masses in our Poulton laboratory and prepared for digital pathology evaluation. Multiple sections were prepared through the larger mass and show an area of marked haemorrhage associated with proliferation of well-differentiated adipocytes (Fig. 2) and abundant, variably sized haemopoietic cells (Fig. 3) to create a densely cellular nodular mass within splenic parenchyma. The haemopoietic cells are very mixed with only occasional mitotic figures. In some areas there are increased numbers of haemosiderophages. The mass is poorly demarcated and merges with surrounding parenchyma.
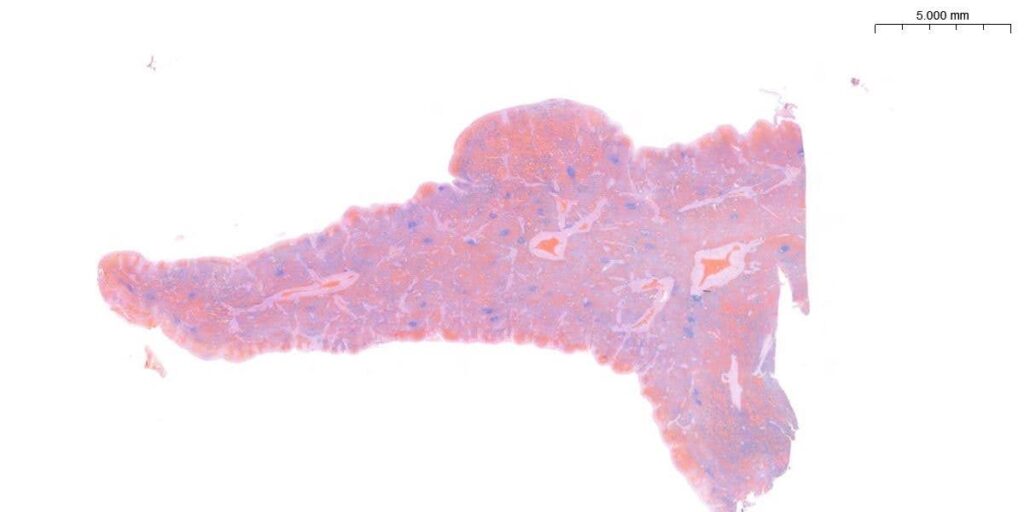
Throughout the spleen there are also occasional smaller foci of adipocytes and nodular masses of proliferating and expansile splenic parenchyma associated with some interstitial haemorrhage. These are relatively discrete masses which expand the capsule and merge with the surrounding parenchyma (Fig 4.). There is some subcapsular distension of vascular sinusoids suggesting congestion. There is no convincing evidence of malignancy in any of the sections examined.
A diagnosis of haemorrhagic splenic myelolipoma and multifocal nodular hyperplasia was made and could be appreciated in the digital pathology sections. The benefit of using this technology was that sub gross evaluation of the tissue could be seen easily, directing the pathologist’s eye to areas of interest. In a tissue such as the spleen, additional software tools can be employed to make sure that all areas of the tissue are examined and none are overlooked. This is especially useful in tissues such as lymphoreticular tissues, where there is increased cell density of the tissue.
Myelolipomas are benign masses composed of admixed adipocytes and normal haemopoietic cells. They are most often found in the spleen, adrenal gland and, rarely, the liver of adult dogs. There is some debate as to whether splenic myelolipoma is a neoplastic, metaplastic or hamartomous lesion. Some grow to a large size and form a space occupying neoplastic-like lesion whilst others are small and multiple. There are no specific clinical signs, and most lesions are typically incidental. Although these lesions are not generally associated with haematoma formation, intratumoural haemorrhage has been reported and may be associated with anaemia, vomiting, anorexia, weight-loss and abdominal distension.
Splenic nodular hyperplasia is a common benign lesion of the spleen of older dogs. Haemorrhage and haematomas can develop within some nodules which can demonstrate a mixture of lymphoid, haemopoietic and stromal hyperplasia and nodules can obtain a large size. Necrosis and inflammation can develop and may represent areas of compromised blood supply in very large nodules. Such lesions are often clinically asymptomatic or can present with vague clinical signs until there is rupture or a critical mass is reached, which causes clinically significant haematological changes. Such nodules can develop as single or multiple foci. In most cases splenectomy is expected to provide a favourable prognosis.
Ben recovered uneventfully from the surgery and is clinically normal 5 months post-surgery.