NationWide Laboratories: case of B cell lymphoma in an 8-year-old entire male border collie

Author: Dr Stacey A Newton BVSc FRCPath CertEM (Int Med) PhD MRCVS
An 8-year-old entire male border collie was presented with enlarged peripheral lymph nodes. No other history was supplied. FNAs from the left submandibular, right prescapular and right popliteal lymph nodes were sent for cytological examination.
All sites demonstrated as similar cytological appearance. The overall population were lymphoid with a predominance of large lymphocytes. Fewer intermediate sized lymphocytes were present with rare small mature lymphocytes. Intermediate and large lymphocytes had round to slightly irregular nuclei with single or multiple varying sized and shaped prominent nucleoli. Some cells had a single large central nucleolus. They had low to slightly increased amounts of dark finely granular basophilic cytoplasm. Some cells had a few clear vacuoles in the cytoplasm and there were a few cells with a clear area to one side of the nucleus. Lymphoglandular bodies were frequent. Occasional mitotic figures were observed.
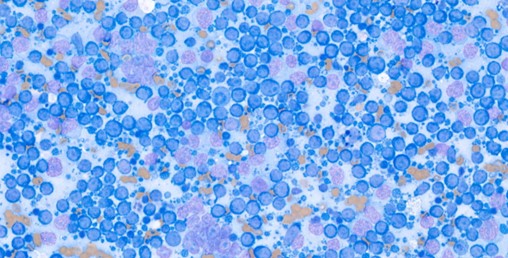
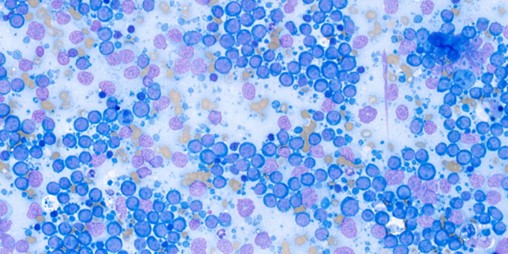
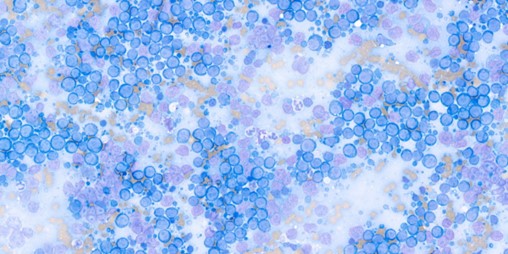
A diagnosis of large cell lymphoma was made.
Further clarification of the type of lymphoma was recommended with either immunocytochemistry, flow cytometry or histology.
The first technique can be performed on the already submitted cytology slides whereas the other two methods required further sampling.
In this case the samples were sent for immunocytochemistry to further classify the lymphoma.
The results of the immunocytochemistry were as follows:
Immunocytochemistry for CD3 and CD20 was performed on the submitted sample. The neoplastic lymphocytes exhibit strong cytoplasmic to membranous staining for CD20 and are negative for CD3. The control slides are appropriately positive.
Interpretation: CD20 positive B cell lymphoma, peripheral lymph nodes
Comments: The ICC findings are consistent with a CD20 positive (CD3 negative) B cell phenotype lymphoma.
Immunophenotyping in the case of lymphoma can be performed using the three techniques indicated above.
This is useful to determine the cell types i.e. B or T cells, present and thus allow selection of appropriate treatments and gives information on prognosis.
Once there is a strong suspicion or confirmation of lymphoma, a full work up of the patient is usually performed to fully stage and assess the disease. This includes full blood work, FNAs for cytology and/or biopsy and imaging (ultrasound and/or thoracic radiographs). Molecular diagnostics (immunohistochemistry, immunocytochemistry, PCR for antigen receptor rearrangement, flow cytometry, and genomic profiling) are used to determine the nature and extent of disease.
Staging (I-V), substaging, cell size/grading of the disease and immunophenotyping are performed.
Most cases are at least stage III if presented with generalized peripheral lymphadenopathy. Stage IV involves hepatosplenic involvement, and stage V refers to the presence of bone marrow infiltration or involvement of extranodal sites like the kidneys, lungs, CNS, or eyes.
B cell is the most common intermediate to high-grade form, whereas T-cell lymphoma is less common but more frequently seen in breeds like Boxers, Golden Retrievers, and Siberian Huskies. T-cell disease is associated with certain anatomic forms, including cutaneous, mediastinal, hepatic, and gastrointestinal.
Treatment
The most common chemotherapeutic profile used in dogs is the doxorubicin-based combination chemotherapy, or CHOP. This consists of 4 drugs that make up the protocol: cyclophosphamide, hydroxydaunorubicin (doxorubicin), Oncovin (vincristine), and prednisone.
References:
M. Zandvliet, Canine lymphoma: a review, Pages 76-104, Published online: 08 Mar 2016, https://doi.org/10.1080/01652176.2016.1152633