Unpicking the puzzle of tick-borne disease
Author: Jana Leontescu
Tick-borne diseases are on the rise in the UK, driven by a combination of environmental and human factors. Climate change is expanding tick habitats and extending their seasonal activity, reshaping the distribution of both endemic and non-native species. Alongside this, the growing popularity of pet travel and the rehoming of dogs from overseas rescue charities continue to introduce animals that may carry exotic ticks and the pathogens they transmit.
Historically, UK concerns focused on Ixodes ricinus and the spread of Lyme disease (caused by Borrelia burgdorferi). But the picture is changing and species that were once confined to the European mainland are now being identified on UK soil.
A thorough history and physical examination remain essential, but laboratory diagnostics -particularly PCR testing – are increasingly important in identifying infections early. Screening may be especially beneficial in imported dogs or those with unexplained haematological or systemic signs.
A shifting landscape
Despite Brexit, dog importation to the UK remains high. Many animals arrive from southern and eastern Europe where a range of exotic tick species and tick-borne pathogens are endemic. These include Ehrlichia canis, Babesia canis, Anaplasma platys and Hepatozoon canis. Some of these pathogens can establish carrier states, with animals appearing clinically normal on arrival but capable of developing clinical disease weeks to months later.
Surveillance data and case reports have confirmed that several exotic tick species and pathogens have already been introduced into the UK and in some cases local transmission of
infection has occurred. For example, an outbreak of Babesia canis in Essex in 2016 highlighted the potential for sustained UK transmission.1
Even without taking more exotic tick species into consideration, the UK is already home to at least 20 native tick species,2 with Ixodes ricinus (commonly known as the sheep or deer tick) being the most widespread and relevant to veterinary and public health (Table 1).3
| Tick species | UK presence | Pathogens transmitted |
| Ixodes ricinus (the sheep tick) | Endemic across the UK | Borrelia burgdorferi; Anaplasma phagocytophilum |
| Dermacentor reticularis (the ornate dog tick) | Established foci in Wales, Devon, Essex, London | Babesia canis |
| Rhipicephalus sanguineus (brown dog tick) | Imported on dogs; survives indoors | Hepatozoon canis; Ehrlichia canis; Anaplasma platys |
Table 1. Key tick species in the UK and the pathogens they transmit.
Clinical signs and diagnostic screening
Tick-borne diseases are challenging to diagnose based on clinical signs alone, especially as many animals – particularly imported dogs – may be subclinical carriers. However, when clinical disease is present, signs can range from mild and non-specific – such as lethargy, pyrexia and lymphadenopathy – to severe and life-threatening. Babesia spp. infections, for example, may result in icterus due to intravascular haemolysis and there may be other complications including prolonged bleeding, petechiae or ecchymoses and neurological signs. A thorough diagnostic work-up, including routine biochemistry and haematology, is essential to identify the underlying cause and guide appropriate treatment.
Haematological and biochemical abnormalities in tick-borne disease
Clinico-pathological changes are variable but may include:
– Anaemia
– Thrombocytopaenia
– Prolonged clotting times
– Azotaemia
– Elevated liver enzymes
– Hypoalbuminaemia
– Hyperglobulinaemia
The role of PCR in diagnosis
Quantitative PCR (qPCR) testing has become an essential tool in the investigation of suspected tick-borne disease. By detecting the presence of pathogen DNA, it confirms active infection at the time of sampling – unlike serology, which reflects prior exposure.
The qPCR is highly sensitive and specific, and when used early in the course of disease, it can detect pathogens before the animal has mounted an antibody response. Many veterinary laboratories offer pathogen-specific or multiple tick-borne disease panels, allowing detection of Babesia spp., Ehrlichia spp,, Anaplasma spp. and Hepatozoon spp. from a single EDTA blood sample.
Lyme disease prevalence, pitfalls and PCR
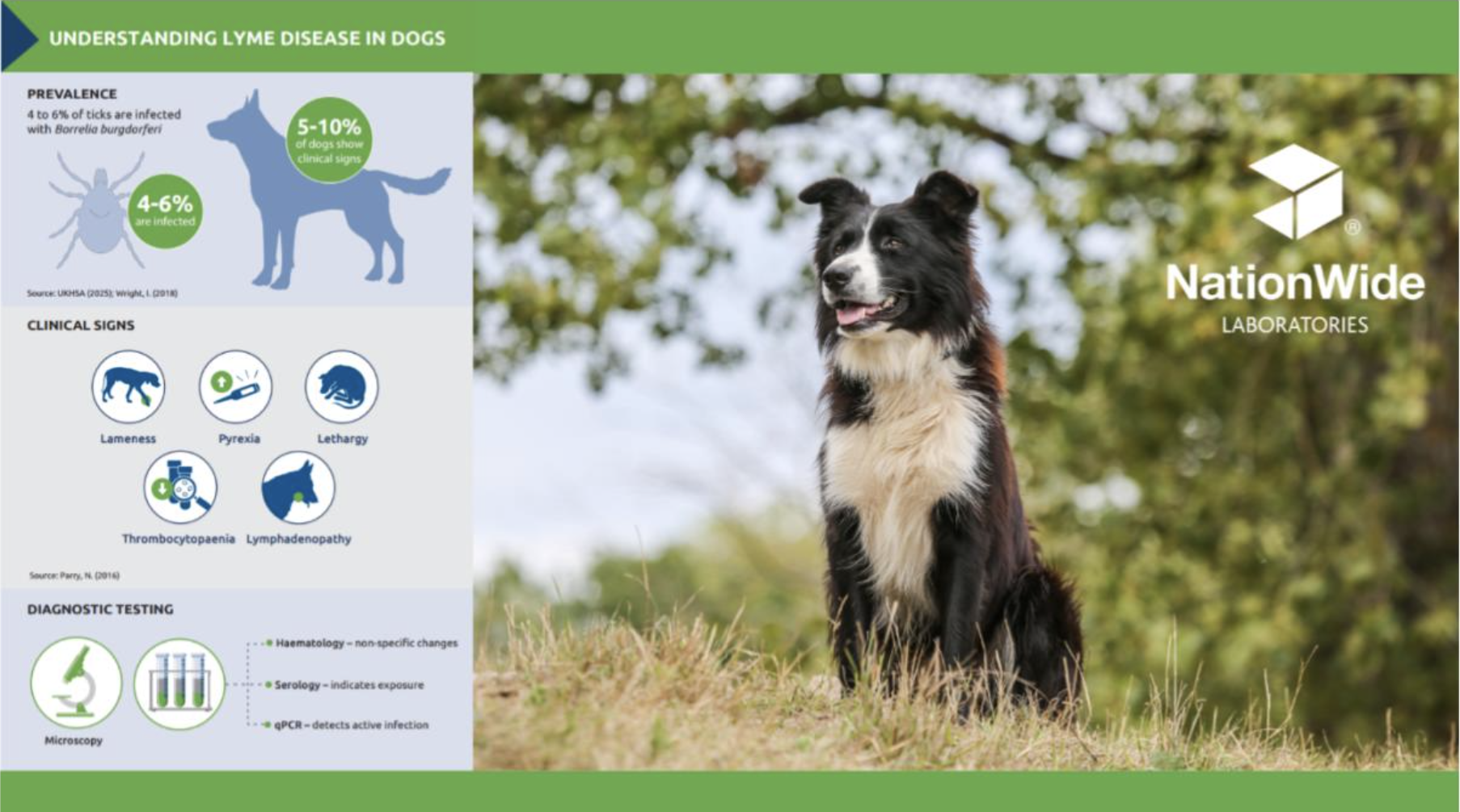
Lyme disease, caused by the spirochaete, Borrelia burgdorferi, remains the most prevalent tick-borne infection in the UK. Transmission is primarily by Ixodes Ricinus, with 4 to 6% of ticks infected.4 And while it is a zoonotic disease of public health significance, the clinical picture in dogs is complex.
Serology is useful in the investigation of Lyme disease. However, the presence of an antibody titre only demonstrates exposure and does not confirm a diagnosis. Correlation with the clinical picture and PCR is recommended. Where there is a high index of suspicion, a negative titre should be followed by repeat sampling in two weeks. If there is no antibody production by around one month after onset of signs then Lyme disease is unlikely.
Most seropositive dogs remain asymptomatic, with only 5 to 10% estimated to develop clinical signs such as, lethargy and pyrexia.5 This high proportion of cases remaining subclinical means the true exposure prevalence in the canine population may be underestimated. Although cats may also be seropositive, it is currently uncertain whether Borrelia infection causes clinical illness in this species.6
Babesia in focus
Another tick-borne disease of significance in the UK is babesiosis. Although Babesia-infected ticks are less commonly encountered than those infected with Borrelia spp., localised areas with higher risk may exist.7 Five Babesia species are known to affect dogs – B. canis, B. vogeli, B. rossi, B. gibsoni and B. vulpes sp. Nov. The most pathogenic and widespread of these is B. canis.8 Diagnosis is traditionally based on clinical presentation along with identification of organisms on blood smear examination. It is worth noting that Babesia trophozoites and merozoites within erythrocytes are more commonly identified on smears made from capillary blood rather than venous blood – the ear pinna offers a suitable site for sampling.
However, in chronic cases or less virulent species – B. canis canis or B. canis vogeli. for example – infection may be below the limit of detection by microscopy. In this situation, PCR testing is recommended due to its high sensitivity and accuracy in diagnosing canine babesiosis.
Emerging and imported infections
Other tick-borne infections that are becoming increasingly important include Ehrlichia canis and Anaplasma species. E. canis is not endemic in the UK but may be seen in imported dogs. The infection is transmitted by Rhipicephalus sanguineus, the brown dog tick which is not established outdoors in the UK but can survive and reproduce indoors. Autochthonous (or local) transmission is theoretically possible indoors if both, infected ticks, and susceptible hosts, are present. Diagnostic tests include blood film examination and PCR testing.
Co-infection and diagnostic clarity
Tick-borne pathogens do not always occur in isolation. In dogs – especially those imported from endemic areas – co-infections with Babesia, Ehrlichia, and Anaplasma species are common
and can significantly influence both clinical presentation and response to treatment. Immunosuppression from one pathogen may exacerbate disease caused by another, and overlapping signs can complicate diagnosis. This underscores the value of comprehensive screening using multiplex qPCR panels, which allow simultaneous detection of multiple vector-borne pathogens from a single blood sample.
With growing numbers of imported animals and an evolving UK tick landscape, tick-borne diseases should now be part of everyday differential lists. A thorough history, awareness of regional risks, and timely access to PCR testing can help clinicians identify infections early, even in subclinical carriers. Whether imported, emerging or endemic, a proactive diagnostic approach is essential.
About the author
Jana Leontescu DVM, MRCVS is a qualified veterinary surgeon with a background in clinical practice in both Romania and the UK. Her interest in veterinary science led her to transition from practice to diagnostic pathology, joining NationWide Laboratories as part of the microbiology team with a focus on parasitology. Now training as a Clinical Pathologist, she is working towards board certification, expanding her expertise in laboratory diagnostics across a range of disciplines. Her experience on both sides of veterinary medicine gives her a well-rounded perspective on the challenges of diagnosing and managing disease.
References
1. De Marco, M.d.M.F., et al. (2017) Emergence of Babesia canis in southern England. Parasites Vectors 10, 241 https://doi.org/10.1186/s13071-017-2178-5
2. Johnson, N. et al. (2022). One Health Approach to Tick and Tick-Borne Disease Surveillance in the United Kingdom. International Journal of Environmental Research and Public Health. 19. 5833. 10.3390/ijerph19105833.
3. Abdullah, S., Helps, C., Tasker, S., Newbury, H., & Wall, R. (2018). Prevalence and distribution of Borrelia and Babesia species in ticks feeding on dogs in the U.K. Medical and Veterinary Entomology, 32(1), 14–22. 4. National Tick Survey 2025. UK Health Security Agency. National Tick Survey – GOV.UK
5. Wright, I. (2018) The risk of Lyme disease exposure to UK dogs. Improve Veterinary Practice.
6. Littman, M. P. et al. (2018). ACVIM consensus update on Lyme borreliosis in dogs and cats. Journal of veterinary internal medicine, 32(3), 887–903. https://doi.org/10.1111/jvim.15085
7. Gandy, S. et al. (2024). Detection of Babesia species in questing Ixodes ricinus ticks in England and Wales, Ticks Tick Borne Dis 15(1): 102291. https://doi.org/10.1016/j.ttbdis.2023.102291
8. Sands, B. et al. (2022) Prevalence of Babesia spp. Pathogens in the ticks Dermacentoe reticulatus and Ixodes Ricinus in the UK. Acta Tropica. Volume 235 https://doi.org/10.1016/j.actatropica.2022.106692 Original publication: Veterinary Edge, issue 53, July 2025, pp 34-36